Uterine tumors are rare in dogs and cats. Uterine tumors account for 0.3% to 0.4% of all canine tumors [1] and 0.29% of all feline tumors [2]. Adenocarcinoma and leiomyoma are the most commonly reported feline uterine tumors [2]. Adenoma, leiomyosarcoma, and lymphosarcoma of the feline uterus have also been reported. One uterine leiomyosarcoma was reported in a study of 13 cats with uterine neoplasia [2], and 4 cases of feline uterine leiomyosarcoma were described in other reports [3,4]; all of 5 cats were over 10 years old at diagnosis. No specific breed predilections have been reported. The clinical signs of feline uterine tumors are abnormal estrus cycles and vaginal discharge; however, the presentation can be non-specific, including weight loss, stranguria, constipation, abdominal distension, and vomiting [1,3]. Although the definitive diagnosis is confirmed by histopathologic examination, radiography, ultrasonography, and computed tomography (CT) are helpful for making the diagnosis, especially in patients with non-specific clinical signs. This case report describes the diagnostic imaging and treatment of uterine leiomyosarcoma in a cat.
A 16-year-old, intact female, domestic short hair cat was presented with 2-week history of anorexia, lethargy, and weight loss from 4.0 kg to 2.65 kg. Physical examination revealed depression and slight icterus. There was no enlargement of the superficial lymph nodes. The complete blood count was unremarkable. Serum chemistry showed increased alanine transaminase (775 U/L, reference range 12-130 U/L), alkaline phosphatase (175 U/L, reference range 14-111 U/L), and total bilirubin (6.3 mg/dL, reference range 0.1-0.5 mg/dL).
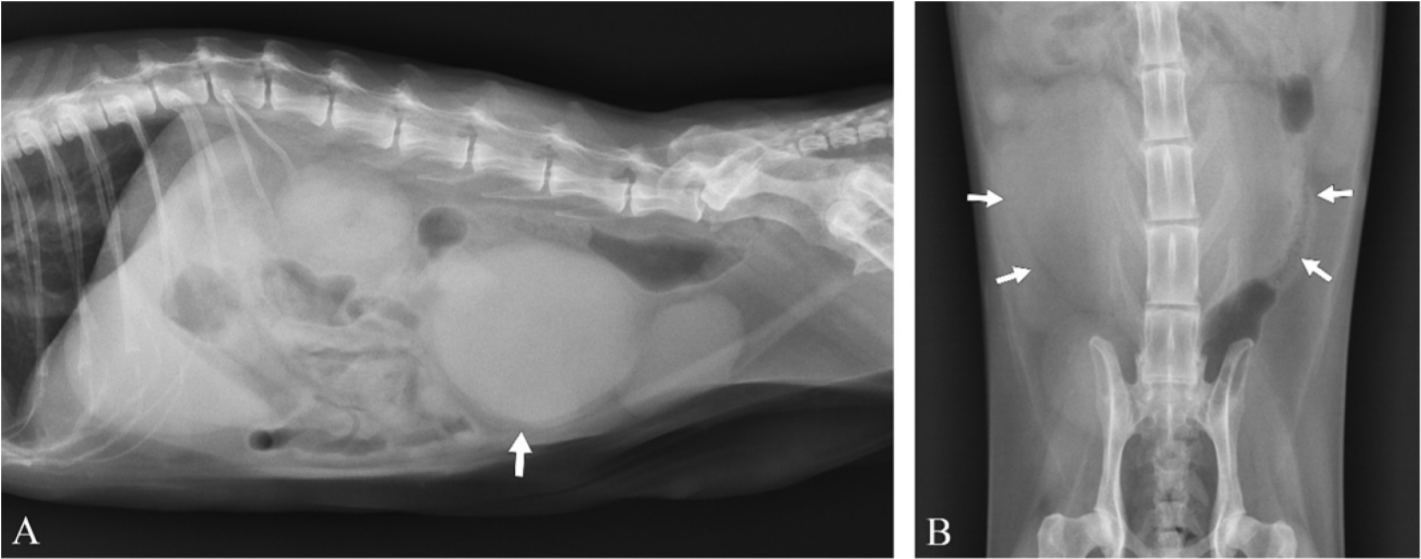
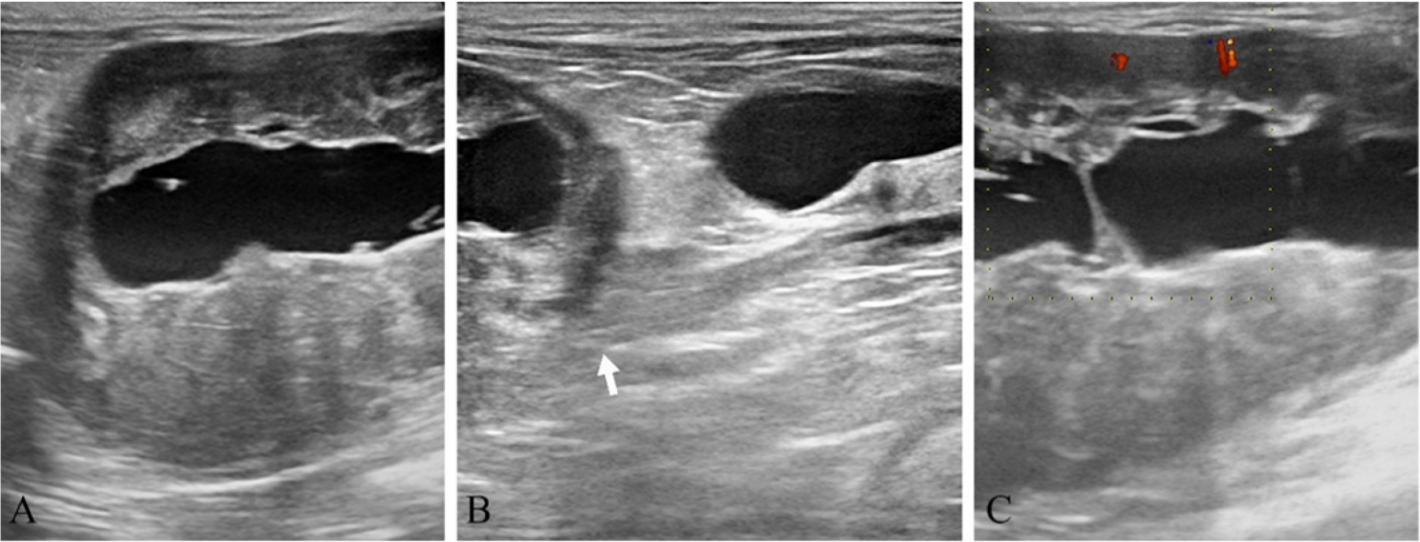
Abdominal radiography identified a large, soft-tissue opacity, heart-shaped mass between the descending colon and urinary bladder, cranially displacing the small intestine (Fig. 1). There were no significant findings on thoracic radiography. Abdominal ultrasonography revealed a heterogeneously hypoechoic mass connected to the vagina, containing anechoic fluid (Fig. 2A, B). Color Doppler sonogram showed mild peripheral vascularization of the mass (Fig. 2C). Both ovaries were enlarged and had anechoic follicles.
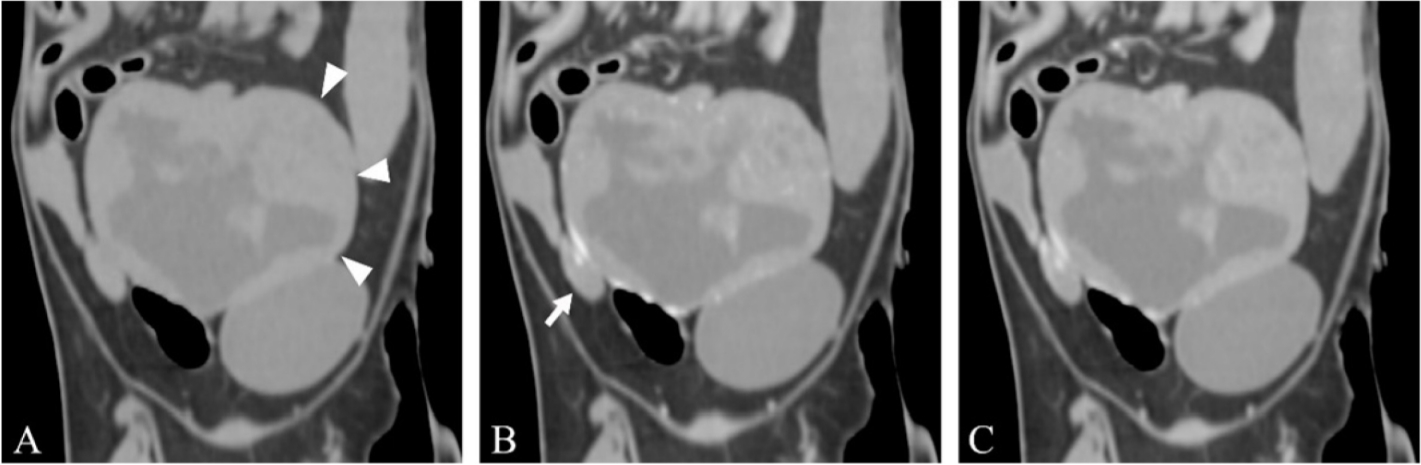
CT examination was performed using a 32-Multislice CT (AlexionTM; Toshiba, Japan). The patient was positioned in dorsal recumbency on the CT table under general anesthesia. The scanning parameters were as follows: 120 kV, 200 mA, 1.0 mm slice thickness, and 0.75 sec rotation time. A contrast study was performed after intravenous injection of 600 mgI/kg iohexol (Bonorex 300 Inj.; Daehan Pharm, Korea) for 20 sec using an autoinjector. Early- and delayed-phase postcontrast CT images were obtained 30 and 90 sec after injection. A severely enlarged (68.3 × 57.4 × 45.0 mm), fluid-filled uterus with an irregularly thickened uterine wall was identified. On postcontrast study, the uterine wall showed heterogeneous contrast enhancement in early- and delayed-phase and the intraluminal fluid showed no contrast enhancement (Fig. 3). Both ovaries were enlarged with multiple follicles. The left kidney and small intestine were displaced cranially by the enlarged uterus. There was no evidence of abdominal regional lymphadenopathy or pulmonary metastasis. Based on radiography, ultrasound, and CT findings, the presumptive diagnosis was uterine tumor without metastasis.
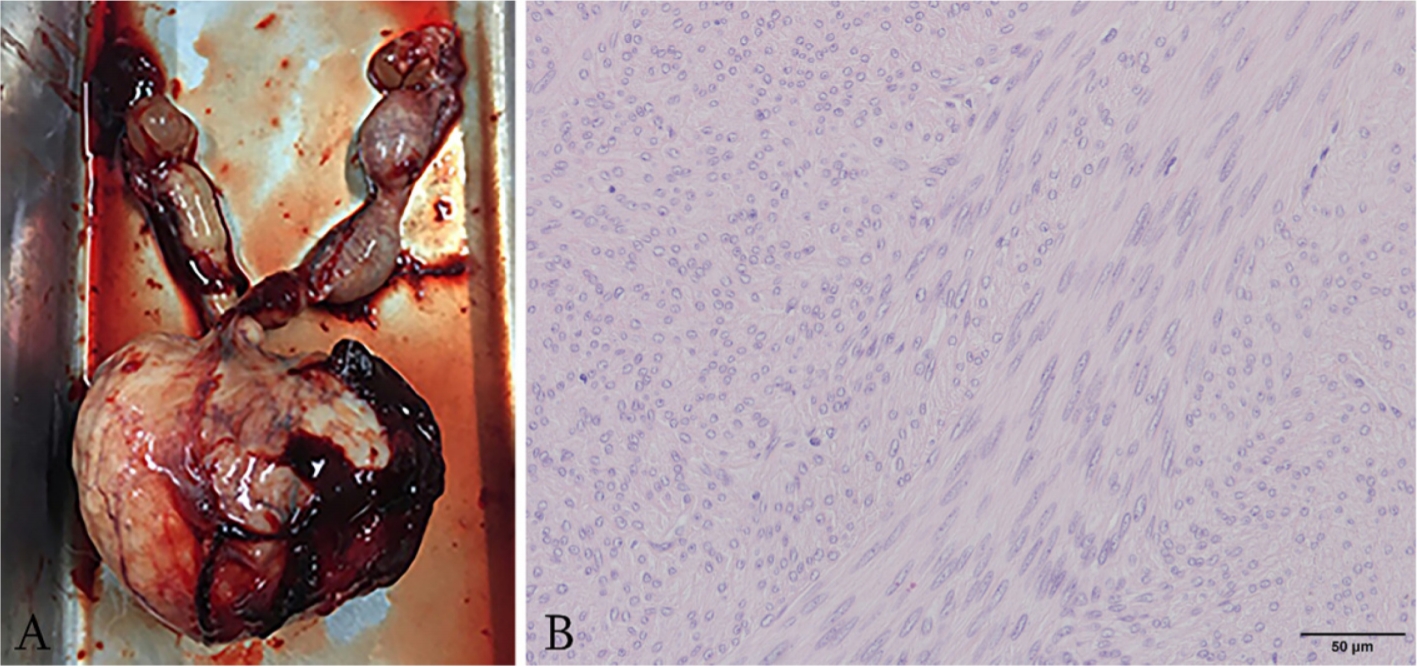
Ovariohysterectomy was performed and postoperative histopathologic diagnosis of the mass was uterine leiomyosarcoma with pyometra (Fig. 4). Spindle cells with elongated, blunt-ended nuclei with granular chromatin, and abundant eosinophilic cytoplasm were found with moderate anisokaryosis. Densely arranged, mildly pleomorphic ovoid to spindle cells with intensely eosinophilic cytoplasm were also detected. Medical treatment for icterus was also performed. After surgery and hospitalization, the clinical symptoms resolved. No notable abnormalities were observed after 1 year of postoperative follow-up.
Differentiation between leiomyoma and leiomyosarcoma is important for selecting from among the available conservative and surgical treatment modalities [5]. Also, presurgical awareness of possible leiomyosarcoma would help in treatment planning [5]. On ultrasonography, uterine leiomyosarcoma appears as a heterogeneous mass containing an anechoic area and hyperechoic foci [6]. However, ultrasonographic features of uterine leiomyosarcoma are similar to those of uterine leiomyoma, which show isoechoic to surrounding uterine tissue with or without anechoic cyst-like lesions and hyperechoic foci [6,7]. It would, therefore, appear that it is not possible to differentiate leiomyosarcoma and leiomyoma from their ultrasonographic appearance alone [7]. In human medicine, color Doppler sonography has been reported to be effective in distinguishing uterine leiomyosarcoma from leiomyoma, although this is still controversial [5]. In a previous study comparing gray-scale and color Doppler sonography to differentiate uterine leiomyoma from leiomyosarcoma, the peripheral vascularity of leiomyoma was increased compared to that of normal myometrium and to that of the center of the tumor. In contrast, uterine leiomyosarcoma had a vascular distribution characterized by increased central vascularity [5]. In our study, mild peripheral vascularity of the uterus was detected, which differ from the results of the previous study in humans. Doppler sonographic studies to differentiate benign and malignant uterine tumors in small animals are lacking; further color Doppler ultrasonographic studies are warranted.
CT features of uterine leiomyosarcoma cases have not been reported in dogs and cats, but there are several reports in humans [8-10]. Uterine leiomyosarcoma in women appears as a large, slightly heterogeneous mass replacing normal uterus, with obvious enhancement and peripheral necrosis on early-phase contrast [9]. However, the CT features of leiomyosarcoma are non-specific compared to those of leiomyomas, lymphoma, and other types of sarcoma in humans [10]. Although other pathologic processes may resemble some of the CT findings of leiomyosarcoma, CT examination is still valuable for detecting the presence of pulmonary, mesenteric, omental, nodal, or soft-tissue metastases [10].
Previous feline malignant uterine tumors showed poor prognosis, in contrast to canine uterine leiomyosarcomas without metastasis reported good prognosis [2,11,12]. In previous studies, there were 1 feline uterine leiomyosarcoma without metastasis [2], and 4 feline uterine leiomyosarcomas with metastasis [3,4]. Among the previous cases of feline uterine leiomyosarcomas, the outcomes of 2 cats were reported: one cat was euthanized and no metastasis was found at necropsy [2]; the other was also euthanized because of abdominal metastasis found 1 month after ovariohysterectomy [3]. The cat in the present study had no evidence of metastasis of the time of diagnosis, which connoted a good prognosis. Data on the prognosis of cats with uterine tumors are scarce [2,3]. The present study adds to the limited available information for determining the prognosis of uterine leiomyosarcoma in cats.
Several reports in dogs have indicated that muscle tumors of the uterus, including leiomyosarcoma and leiomyoma, may play a role in the pathogenesis of pyometra. In a previous report, a correlation between canine uterine leiomyosarcoma and pyometra was observed [6]. The possibility of a predisposition to infections was ascribed to immunosuppression and loss of local defense mechanisms by the malignant mass [6]. Further, uterine leiomyoma obstructs the cervix, and pyometra is caused by impairment of natural drainage of the cervix in dogs [13,14]. Similarly, in the present case, uterine leiomyosarcoma with pyometra was confirmed.
In conclusion, this is the first report describing the CT features of a rare case of uterine leiomyosarcoma in a cat. Diagnostic imaging including radiography, ultrasonography, and CT is useful for determining tumor origin and metastasis. The prognosis of uterine leiomyosarcoma without metastasis may be good after complete surgical resection, even if the tumor is malignant.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print







