Prevalence, species, and antimicrobial resistance of Acinetobacter in surgical practice and laboratory dog husbandry room environments
Article information

Abstract
Acinetobacter is a bacteria found in the environment and clinical specimens, causing nosocomial infection and antimicrobial resistance (AMR) threats. This study examined the prevalence, species, and AMR characteristics of Acinetobacter isolated from surgical practice and the laboratory dog husbandry room environments (n = 235) at Rajamangala University of Technology Tawan-ok veterinary hospital during 2018-2019. The prevalence of Acinetobacter in the laboratory dog husbandry room and veterinary belongings were 2.55% and 0.43%, respectively. Species determination was Acinetobacter hemolyticus (2.13%) and Acinetobacter baumannii (0.43%) from environments in the laboratory dog husbandry room, and Acinetobacter junii (0.43%) from the shoes used in the surgical practice room. AMR was observed in both study environments and the specimens sent to the Veterinary Diagnostic Center. These isolates had a high resistant percentage to amoxicillin-clavulanic acid (84.62%), sulfamethoxazole-trimethoprim (61.54%), and cephalexin (53.85%) but were susceptible to imipenem. Compared to the isolates recovered from the clinical specimens, most isolates derived from environments exhibited multidrug resistance and shared correlated resistance patterns. These results highlight the need for sanitization in the dog husbandry room. Furthermore, the AMR results can be used as a preliminary baseline for studying AMR Acinetobacter contamination in animals and their environments.
Introduction
Acinetobacter is gram-negative coccobacilli or short rods in the family Moraxellaceae [1], which can be found in water, soil, sewage, and foods, as well as in the skin and mucous membranes of humans and animals [2,3]. This group of bacteria recently has an impact on public health because they are considered as the source of antimicrobial resistance (AMR) and multidrug resistance (MDR), particularly for carbapenems, which cause difficulties in treatment and result in a high mortality rate [4]. Since 1988, Acinetobacter has comprised 10% of bacteria found frequently as nosocomial infections in the United States and worldwide [5].
In Thailand, the incidence of Acinetobacter infections in hospitals increased from 2%-4% to 10%-30% for the last decade, particularly in the ward unit [6]. The National Anti-microbial Resistant Surveillance Center Thailand also reported that the resistance rates of Acinetobacter spp. to antimicrobial agents increased gradually during 2000-2020 [7]. In addition, Acinetobacter was found mostly as contamination on nurses’ hands [8], and can be isolated from the soil, water, air, sink, urine bottle, bed, and respiratory equipment in hospitals [9,10]. Clinical specimens, such as urine, exudate, respiratory tract, and blood samples, are a major source of Acinetobacter infection [11,12]. Moreover, Acinetobacter baumannii is the main causative agent usually recovered from human clinical cases [6].
In addition to human hospitals, Acinetobacter can often be found in clinical specimens of animals [13]. Among several species, A. baumannii is important in animal hospitals underlying severe illnesses, such as canine pyoderma, urinary tract infection, and foal sepsis, as well as AMR infections [6,14]. Based on a study in Germany during 2000-2008 [15], MDR A. baumannii isolates recovered from veterinary hospitals and clinics were distinctly resistant to carbapenem groups, such as human cases [16].
Other species of Acinetobacter, which are not A. baumannii (non-baumannii Acinetobacter), including Acinetobacter pittii, Acinetobacter calcoaceticus, Acinetobacter bereziniae, Acinetobacter hemolyticus, Acinetobacter johnsonii, Acinetobacter lwoffii, Acinetobacter schindleri, Acinetobacter radioresistens, Acinetobacter beijerinckii, Acinetobacter junii, Acinetobacter generi, and Acinetobacter ursingii have also been reported in animals particularly in livestock, horses, and pets [13,17]. Some outstanding species, such as A. hemolyticus, were found in the general environment and tended to cause severe clinical cases concerned with the environment in hospitals. On the other hand, AMR, particularly carbapenems, was not determined clearly [18]. A. junii has been reported in calculi obstructions in the ureter [19]. As mentioned previously, Acinetobacter is found mainly in nature. Nevertheless, few studies have been conducted on the epidemiology and pathogenesis in the environment [2], leading to gaps of knowledge about the relationship of this bacteria in humans, animals, the environment, and the loss of AMR transferring pathways [14,16].
According to the gaps, this study focused on the prevalence of all Acinetobacter species and their AMR patterns recovered from surgical practice and laboratory dog husbandry room environments at the veterinary hospital, Rajamangala University of Technology Tawan-ok. Furthermore, the AMR patterns from the study environment were compared with the same bacterial group isolated from clinical specimens sent for analysis at Veterinary Diagnostic Center, Faculty of Veterinary Medicine, Rajamangala University of Technology Tawan-ok during 2016-2020. These results can be used as baseline data in the study of AMR Acinetobacter in animals, humans, and the environment.
Materials and Methods
Sample collection
This study was a descriptive research. Two hundred and thirty-five swabbed samples from the surgical practice and laboratory dog husbandry room at the veterinary hospital, Rajamangala University of Technology Tawan-ok, Chonburi province, Thailand, between January 2019 and March 2020. The samples were composed of four categories: laboratory dog husbandry room environment, such as floor under cages, the inner area of cages, dog beds, pet food cabinet, room floor, sewer pipe, sink, and storage area floor (n = 100); laboratory dogs, such as oral mucous membrane, anus, blood, saliva, leash, collar, feeding bowl, skin swab, and cotton containing alcohol used in skin scrub (n = 80); veterinary belongings, including shoes used in the surgical practice room, used syringe and needle (n = 35), and hands of people in contact with dogs (n = 20).
Acinetobacter isolation
All samples were taken for bacterial isolation and biochemical tests applied from previous studies [20-23]. Briefly, swabbed samples were cultured on tryptic soy broth (TSB) and incubated at 37°C and 44°C for 24 to 48 hours. The turbid TSB was then transferred to culture on MacConkey agar and incubated under the same conditions above. Subsequently, a single typical (pale pink or colorless) colony was transferred from MacConkey agar and identified by gram staining, motility, morphology, and oxidation/fermentation tests. Moreover, biochemical tests [21,24] were applied for species confirmation. The species of all confirmed Acinetobacter isolates were recorded and stored for further analysis.
Antimicrobial susceptibility testing
All Acinetobacter isolates were taken to determine the antimicrobial susceptibility test by the disc diffusion method of Kirby-Bauer [25] using data from previous studies [13-15,20] for selected antimicrobial discs. The antimicrobial-resistant percentages were then concluded and compared with Acinetobacter isolates derived from the clinical specimens of the Veterinary Diagnostic Center, which had been reported in 2016-2020.
Statistical analysis
Statistical analysis was applied to determine the prevalence of Acinetobacter derived from four categories (laboratory dogs husbandry room, laboratory dog, veterinarian belongings, and hands of people in contact with dogs) for the most variables. The analysis with the likelihood ratio test and Fisher’s exact test, using R version 3.1.2 (R Foundation for Statistical Computing, Austria) were applied. The results were reported as the odds ratios (ORs) with the associated 95% confidence interval (CI), and a p-value < 0.05 was considered significant.
Results
Prevalence of Acinetobacter in environments
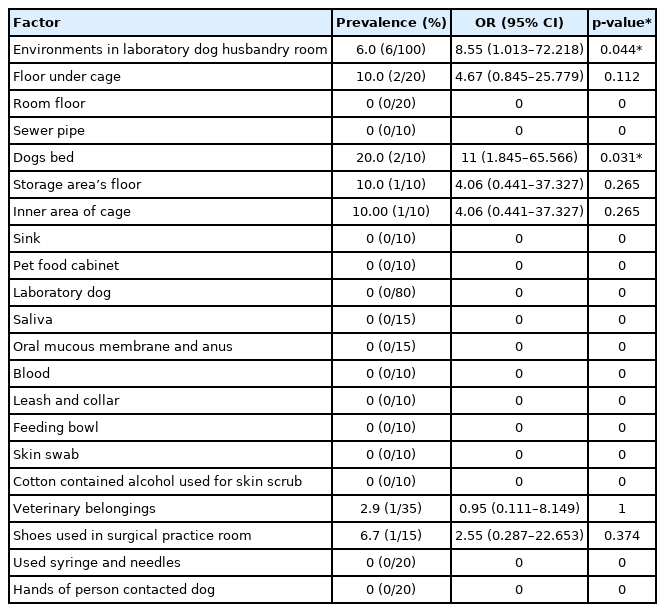
The overall prevalence of Acinetobacter in this study was 2.98% (7/235). Considering the categories, the prevalence in the environments of surgical practice and laboratory dog husbandry rooms were 2.55% (6/235), or 6.0% (6/100) in this category (OR, 8.55; 95% CI, 1.013-72.218; p = 0.044). The veterinary belongings had a 0.43% (1/235) prevalence, or 2.86% (1/35) in this category, while there was no positive sample for Acinetobacter in the laboratory dogs and hands of people in contact with dogs (Table 1). The laboratory dog husbandry room environment showed the highest prevalence, which was determined in the samples from the floor under cages, dogs beds, storage area floor, and inner area of the cages. Significantly, the prevalence in dogs beds was 20.0% (2/10) with OR, 11, which was higher than other factors in laboratory dog husbandry room environment. The odds of Acinetobacter prevalence in the floor under cages, storage area floor, the inner area of the cages, and the shoes used in the surgical practice room were 4.67, 4.06, 4.06, and 2.55, respectively, compared to other factors (Table 1).
Prevalence of Acinetobacter
Species of Acinetobacter isolates
All 235 swabbed samples were determined to be Acinetobacter for seven isolates, including five isolates of A. hemolyticus (2.13%, 5/235) recovered from the floor under cages (0.85%, 2/235), storage area floor (0.4%, 1/235), the inner area of cages (0.43%, 1/235), and dogs’ bed (0.43%, 1/235). One isolate of A. junii (0.43%, 1/235) was recovered from shoes used in the surgical practice room, and one isolate of A. baumannii (0.43%, 1/235) was recovered from a dogs’ bed (Fig. 1).

Percentage of Acinetobacter’s species.
Antimicrobial susceptibility testing
Most Acinetobacter isolates recovered from the environments in surgical practice, the laboratory dog husbandry rooms (6/7), and clinical specimens of Veterinary Diagnostic Center (5/6) were resistant to amoxicillin-clavulanic acid at 84.62%. In contrast, the A. hemolyticus recovered from the storage area floor and A. lwoffii vdc2 from the Veterinary Diagnostic Center were resistant to sulfamethoxazole-trimethoprim. In addition, 61.54% of Acinetobacter isolates were resistant to this antimicrobial type, except for A. hemolyticus and A. baumannii recovered from the dog beds, and A. lwoffii vdc2 was susceptible to this drug (Table 2). Approximately 53.85% of the isolates recovered from the environments in surgical practice and laboratory dog husbandry room (4/7) and clinical specimens of Veterinary Diagnostic Center (3/6) were resistant to cephalexin, except A. hemolyticus recovered from storage area floor and dog beds, A. junii recovered from shoes used in the surgical practice room and A. lwoffii vdc2 (Table 2).

Susceptibility pattern of Acinetobacter isolates to antimicrobial agents
AMR patterns of Acinetobacter
The AMR patterns of Acinetobacter primarily found in this study were amoxicillin-clavulanic acid, cephalexin, and doxycycline (13.04%) of A. hemolyticus isolated from the inner area of cages, the floor under the cage, and vdc2, while amoxicillin-clavulanic acid and sulfamethoxazole-trimethoprim (13.04%) of A. junii recovered from the shoes used in the surgical practice room, A. hemolyticus vdc1 and A. lwoffii vdc1 (Table 3). Another pattern with a high percentage of resistance (13.04%) was clindamycin from A. lwoffii vdc1 and 2 and A. hemolyticus vdc1. Other MDR patterns found mainly in this study (8.70%) were amikacin, amoxicillin-clavulanic acid, cephalexin, and sulfamethoxazole-trimethoprim of A. hemolyticus recovered from the floor under the cages; amoxicillin-clavulanic acid, cephalexin, doxycycline, and sulfamethoxazole-trimethoprim of A. hemolyticus recovered from the inner area of cages and floor under cages; amoxicillin-clavulanic acid, cephalexin, and ceftriaxone of A. baumannii isolated from dogs’ bed and vdc1; amoxicillin-clavulanic acid, cephalexin, and sulfamethoxazole-trimethoprim of A. hemolyticus recovered from the floor under cages and A. johnsoniii vdc1 (Table 3). On the other hand, all Acinetobacter isolates recovered from the environments in surgical practice and laboratory dog husbandry room (7/7) and two isolates from Veterinary Diagnostic Center, including A. hemolyticus vdc2 and A. baumannii vdc1, were susceptible to imipenem (Table 2).
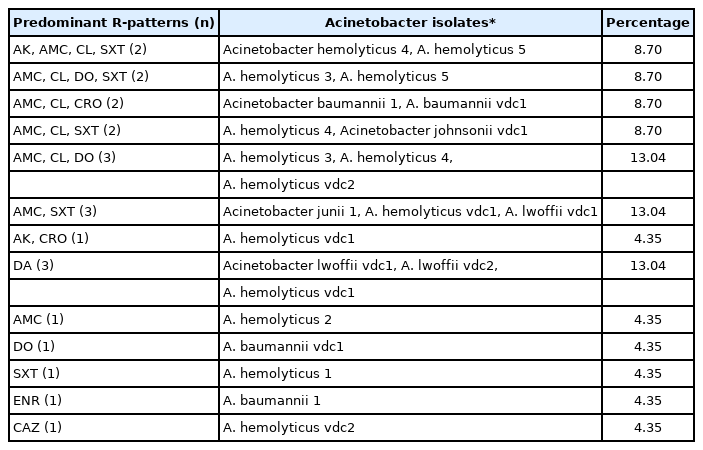
Predominant resistance patterns (R-patterns) of Acinetobacter isolates
Discussion
Prevalence of Acinetobacter in environments
In this study, the prevalence of Acinetobacter in the laboratory dog husbandry rooms environment was 6.0% (Table 1), which was similar to a previous study. Uwingabiye et al. [12] reported that clinical specimens of hospitals showed a prevalence of 6.94%. According to the ORs in Table 1, the prevalence of Acinetobacter in the environment of laboratory dog husbandry rooms was 8.55 times higher than the other factors, including laboratory dogs, veterinary belongings, and people in contact with the dog’s paws. The environment is an intermediate source of bacteria dissemination. Two reports stated that the healthcare environments could be accumulation and multiplication sources of Acinetobacter affecting patients [26,27]. In addition, the dog beds, which are closely in contact with animals, have 11 times the risk of Acinetobacter prevalence compared to other locations in the laboratory dog husbandry room (Table 1). This group of bacteria can survive in many environments and produce biofilms to protect their vegetative cells on both abiotic and biotic surfaces, particularly in A. baumannii, leading to prolonged survival and nosocomial infection [16,27]. This problem would be more severe if the healthcare settings have insufficient sanitization [27].
Unlike the prevalence of A. baumannii recovered from medical equipment, such as respiratory tubes and blood pressure monitors [28], the prevalence in veterinary belongings was only 2.9%. Hence, the highest prevalence was found only in shoes used in the surgical practice room, needles, and syringes but did not cover other veterinary belongings. Moreover, the laboratory dogs in this study were healthy and had no septicemia or severe clinical diseases [13,20]. Therefore, Acinetobacter was not detected in the needles and syringes. Although the shoes used in the surgical practice room had a prevalence of 6.7%, it was assumed that those shoes might have been a reservoir of Acinetobacter [2].
No positive Acinetobacter sample was found in the laboratory dogs, which contrasts with several reports. A study in Reunion Island of France claimed that pets (dogs and cats) were carriers of A. baumannii with a prevalence of 6.5% [29]. Black et al. [30] detected Acinetobacter in 7% in the clinical specimens from the canine intensive care unit and sent for bacterial culture and antimicrobial sensitivity test. On the other hand, some studies explained that healthy laboratory dogs without an immunocompromised state would have a primary line of body defense that could depress the multiplication of undesirable normal flora, such as Acinetobacter spp. [31,32].
Several studies reported that the hands of healthy people could be a multiplication source of A. baumannii spreading to patients, particularly with wounds or injuries on the skin [8,28], which is in contrast to the present study in that no Acinetobacter was found on staff hands. The reason, in this case, might be that people in contact with dogs had a strict handwashing regimen and recognized the importance of hygiene [14]. This suggests that the bacterial transferring pathway between dogs and humans or the environment and humans could be broken by hygiene and sanitation practices [14,20,33].
Species of Acinetobacter isolates
Three species of Acinetobacter were recovered in the environment of this study (Fig. 1). A. hemolyticus has been found in the environment, such as water and human skin [2]. Therefore, this species would be found on the floor under cages, storage area floor, the inner area of cages, and dog beds. The results suggest that dogs roaming outside the building transferred these bacteria from the environment into husbandry rooms. A. junii has been reported in viscous mud, sewage, water, soil, and human skin [2], including animals [17]. The determination of A. junii in shoes used in the surgical practice room might originate from sewage in environmental contamination. A. baumannii can be found in humans, animals, the environment, and medical equipment, including clinical specimens in hospitals and veterinary hospitals [12,13,15,23,28,33]. This species was isolated from dog beds, which were assumed to be contaminated.
Antimicrobial susceptibility testing
According to Table 2, the class of antimicrobials showing a high resistance percentage was the cephalosporin group, including amoxicillin-clavulanic acid (84.62%), cephalexin (53.85%), and ceftriaxone (23.08%). This group of antimicrobials is used frequently in clinics [34]. These results were correlated with previous studies reporting that approximately 90% of this bacteria recovered from clinical specimens and the hospital environment were resistant to both old generation and new broad-spectrum cephalosporins [11,20]. Moreover, 23.08% of Acinetobacter isolates in this study were also resistant to the aminoglycoside drug (amikacin). Recently, these two groups of antimicrobials tended to increase the level of resistance [20].
A. baumannii was considered the most outstanding species of MDR [23,29,33,35]. This species uses various resistant mechanisms to survive against β-lactams and carbapenems, particularly the production of β-lactamase or carbapenemases [13,36]. In agreement with this study, A. baumannii recovered from the dog beds and vdc1 were resistant to amoxicillin-clavulanic acid, cephalexin, and ceftriaxone (Table 3). As mentioned previously, this group of antibiotics is generally used for treatment in animal healthcare [34], which might increase the selection pressure of AMR in the environment leading to horizontal gene transfer [13,33,36]. Amikacin is usually selected to treat MDR Acinetobacter infections [13,28], but most of the Acinetobacter isolates in the present study were susceptible to this drug, except for A. hemolyticus recovered from the floor under the cage and vdc1 (Table 3). Only one isolate of A. baumannii recovered from dog beds in this study was resistant to enrofloxacin, which was the same as the study before. The researchers reported that a small percentage of Acinetobacter isolates were resistant to this drug [13]. Zordan et al. [15] reported that all MDR A. baumannii isolated from veterinary clinics in Germany were resistant to clindamycin. In contrast to the present study, only 13.04% of clindamycin resistance was detected (Table 3). Interestingly, several studies reported the accelerated trend of carbapenems resistance [7,13,16]. On the other hand, there was no resistance to imipenem or carbapenem. These results highlight the need for rational drug use in animal hospitals and livestock production to reduce AMR threats.
AMR patterns of Acinetobacter
This study identified five predominant MDR patterns of Acinetobacter (Table 3) that were resistant to at least three antimicrobial agent groups [37], representing approximately 45.5% of the related isolates. Several species isolated in the environment of this study as well as clinical cases from animal hospitals sent for analysis at the Veterinary Diagnostic Center, including A. hemolyticus, A. baumannii, A. johnsoniii, had MDR patterns. A previous study stated that A. baumannii was mostly found with the MDR patterns of Acinetobacter recovered from all clinical specimens in veterinary hospitals [13]. This contrasts with the present study showing that A. hemolyticus presented the highest frequency of MDR patterns. The MRD Acinetobacter determination in the hospital environment would relate to nosocomial infections and circulate in both human and animal intensive care units [16,35]. On the other hand, AMR gene transmission and resistant mechanisms of Acinetobacter should be considered for further study.
In conclusion, Acinetobacter is a gram-negative bacteria generally found in the environment and clinical specimens of human and veterinary hospitals. In this study, the determination of this bacteria in the environments of laboratory dog husbandry room and veterinary belongings were A. hemolyticus, A. junii, and A. baumannii. The finding emphasizes the importance of sanitary management and cleaning the operating place and laboratory dog husbandry room to reduce the source of bacterial contamination. In addition, most antimicrobial-resistant patterns of the Acinetobacter isolates recovered from surgical practice, and laboratory dog husbandry rooms environments were MDR, which is in agreement with the isolates derived from the clinical specimens of the Veterinary Diagnostic Center. These MDR Acinetobacter determined the public health importance of the environment and its related clinical specimens.
Notes
The authors declare no conflict of interest.
Acknowledgements
This study was supported and encouraged by Faculty of Veterinary Medicine, Rajamangala University of Technology Tawan-ok. We thank the university veterinary hospital for sampling collection, Veterinary Diagnostic Center for data assistance and we appreciate Areeya Sukkasem for hard working in laboratory.