Veterinary management protocol for non-human primates: quarantine, anesthesia, and postoperative care for mastoidectomy at animal research institutions
Article information

Abstract
Non-human primate (NHP) research faces challenges due to zoonosis risk and complex veterinary management yet lacks standardized guidelines for animal care. Therefore, we developed an advanced veterinary management protocol for NHP quarantine, anesthesia, and postoperative care. Three female 4 to 5-year-old cynomolgus monkeys were anesthetized and underwent various tests, including body weight, temperature, blood tests, urinalysis, microbiological monitoring, and physical and dental examinations. Ivermectin and medicated baths were administered to eradicate ectoparasites and endoparasites, and testing was repeated 30 days later. Following quarantine, we performed computed tomography and anesthesia maintenance for mastoidectomy. To relieve pain and maintain body weight, we administered tramadol intramuscularly 4 times/day for 3 days and meloxicam subcutaneously twice daily for 14 days. Feed replacements were provided. During the 33-day quarantine period, physical examinations revealed no abnormalities indicative of infectious diseases, and no specific clinical symptoms were observed. Through a preliminary test of anesthesia time, we selected ketamine 4 mg/kg + medetomidine 50 µg/kg for short experiments such as computed tomography, and ketamine 8 mg/kg + medetomidine 50 µg/kg for intubation. Ten days after mastoidectomy, NHPs consumed 100 kcal/kg and recovered their body weight. This study offers advanced veterinary management guideline for NHP research. Such protocols can lead to more standardized and ethical practices in NHP research, thereby enhancing the quality of studies on NHPs and the translation of findings to human health and disease.
Introduction
Non-human primates (NHPs) play an indispensable role in scientific research, offering valuable insights in preclinical studies. Their remarkable similarities to humans in terms of genetics, behavior, anatomy, and physiology can advance our understanding of human health [1,2].
While rodents are commonly used in preclinical research because of their cost-effectiveness and short life cycle, their significant physiological, pathological, and anatomical differences from humans can lead to erroneous scientific results [3,4].
Considering the complexity of NHPs, they require specialized and comprehensive veterinary management during anesthesia and postoperatively to maintain their physical and psychological health throughout the experiment. However, studies on overall veterinary management, including quarantine, anesthesia, and postoperative care, are lacking.
Zoonotic diseases in NHPs are not limited to wildlife; they also occur in animal research facilities. Shigella flexneri, Mycobacterium tuberculosis, and parasites have been identified in NHPs in research facilities worldwide [5,6]. A 2021 incident at a Chinese animal research facility resulted in a person’s death following an autopsy of 2 monkeys. It was determined that the individual had contracted the Macacine alphaherpesvirus 1 (i.e., B virus) [7]. Such events could have been prevented with a comprehensive NHP quarantine program. Efforts are being made to eliminate zoonotic diseases from NHP populations worldwide. However, animal research institutions have not reported specific quarantine methods. Therefore, it is necessary to enhance our understanding of NHP quarantine through further detailed studies.
Meeting the high demand for breeding, handling, and veterinary management of NHPs is challenging due to their highly advanced sentience, perception, and manual dexterity, which are similar to those of humans [8,9]. Failure to meet strict standards for NHP management can result in elevated stress and self-injurious behavior [10,11].
The management of NHPs in animal research facilities has evolved significantly compared to the past few decades when the complex mental and physiological states of NHPs and the pain induced by experimentation were not adequately considered [12]. NHP researchers are responsible for ensuring that environments in research facilities minimize unnecessary distress and pain for these animals [13]. In particular, captive animals in facilities such as zoos or animal research centers require high-quality care as poor care may influence animal research accuracy and reliability [14,15]. Non-standardized and non-scientific veterinary care can cause pain and stress in animals and alter their physiological parameters [14,16]. Anesthesia, a critical veterinary care aspect, reduces pain and anxiety during surgery, computed tomography (CT), magnetic resonance imaging, and diagnostic tests [17,18]. Its duration should be minimized while ensuring adequate depth to avoid side effects, such as hypotension or cardiac dysfunction. However, since relatively few studies have been conducted on NHPs, data on appropriate anesthesia duration and depth remain scarce. Therefore, selecting the right anesthetic and dose for preclinical studies with NHPs remains challenging.
This study aimed to develop comprehensive guidelines for veterinary management of NHPs, encompassing the complete research process from initiation to completion, for researchers working at animal research institutions. These guidelines aim to improve the overall quality of NHP research by providing safe research practices for beginners and minimizing the stress experienced by NHPs during quarantine, anesthesia, and postoperative care.
Materials and Methods
Animals and ethics statement
Six female cynomolgus monkeys (Macaca fascicularis), aged 4 to 5 years, were obtained from the Primate Resources Center, Korea Research Institute of BioScience & Biotechnology, and were housed at the preclinical research center, K-MEDI hub. Six NHPs were randomly divided into 2 groups, with 3 animals each assigned to the negative and treatment groups.
The animal study protocol was approved by the Institutional Review Board of Daegu Gyeongbuk Medical Innovation Foundation (protocol code DGMIF-21111601 and approval date: October 19, 2022; protocol code KMEDI-2209150 and approval date: September 14, 2022). This study strictly adhered to the American Society of Primatologists’ Principles for the Ethical Treatment of NHPs. All animal experiments were conducted in full compliance with the regulations in the Republic of Korea’s animal protection laws.
Quarantine
Quarantine procedures for NHP researchers
Quarantine, mandatory for both the negative and treatment groups, aimed to prevent zoonotic diseases in primates. Before the research, a program identified potential diseases, and researchers, educated on zoonotic risks like B virus from NHPs, underwent chest radiography in annual health check-ups. The NHP area, with its air conditioning system, was isolated from other animal areas. Researchers underwent an air shower, wore disposable protective gear, and items leaving the NHP area were sterilized. In quarantine, an emergency kit with betadine scrub, antivirals, and antibiotics was available.
Quarantine procedures for NHPs
NHPs were anesthetized with intramuscular 4 mg/kg tiletamine with 2 mg/kg xylazine on a heating blanket to maintain body temperature. As previous study, the combination of tiletamine and xylazine resulted in an average surgical anesthesia duration lasting 72 minutes [19]. A 4 to 5 years-old cynomolgus monkey corresponds to the young adult stage [20]. While neurotoxicity during anesthesia can potentially manifest in very young stages of NHPs, it was considered feasible for the NHPs utilized in this study, which were in the young adult stage. Additionally, they fell within the normal body weight range typically observed in the 4 to 5-year age group, leading to the administration of the appropriate dosage [21,22].
Under anesthesia, body weights were measured, and a 37℃ medicated bath was administered. Blood samples were collected from a saphenous vein, and fecal and urine samples were obtained for comprehensive testing, including complete blood count, biochemical analysis, urinalysis, and microbiological examination for pathogens including B virus, M. tuberculosis, Mycobacterium bovis, varicella-zoster virus, Salmonella spp., Shigella spp., Yersinia spp., ectoparasites, and endoparasites.. In-house testing, including microbiological monitoring, minimized pathogen transmission risk. The purified protein derivative (PPD) skin test for silent tuberculosis was conducted on the right eyelid, with negative results confirmed at 24, 48, and 72 hours post-anesthesia. Other examinations included heart auscultation, rectal thermometer body temperature measurement, SpO2 measurement, dental examination, and 0.2 mg/kg subcutaneous ivermectin administration.The breeding room’s floor and walls were swept and disinfected daily to eradicate potential pathogens.
Daily monitoring and assessment
Daily monitoring included food intake and clinical symptoms such as abnormal behavior. Body weights were measured on the 15th and 30th days. Calorie intake of NHPs was calculated to determine whether they consumed 100 kcal/kg body weight per day [23]. On the 30th day, the monkeys were anesthetized again, and various tests were performed, including complete blood count, biochemical analysis of urine samples, auscultation, body temperature, PPD skin test, and physical examination, except microbiological monitoring. On the 33rd day, all results were analyzed to determine the end of the quarantine period after confirming a negative PPD skin test without anesthesia.
Husbandry
NHPs were housed in an accredited facility (Association for Assessment and Accreditation of Laboratory Animal Care International #001796) and fed a gamma-irradiated Certified Global 20% Protein Primate Diet (#2050; ENVIGO, USA). Respecting NHPs' perceptual abilities, we provided enrichment, offering a floor area of 1.04 m2 per NHP, exceeding the 0.4 m2 global guideline [24]. Cages had mirrors and bars for tree-climbing behavior, with cleaned toys, mirrors, or stainless-steel balls. NHPs received fruits and vegetables alongside their feed. Post-adaptation, a friendly approach like petting or feeding was implemented. When handling NHPs for measurements or injections, neighboring cage views were blocked with a cotton towel.
Anesthesia time
Induction, recovery, and total anesthesia times were measured and modified, following Guedel’s classification to treatment group [25]. We tested the following doses of anesthesia combinations intramuscularly using 3 NHPs at 3-day intervals: 50 µg/kg medetomidine + 4 doses of ketamine (2, 4, 6, or 8 mg/kg). The anesthesia times for 4 mg/kg tiletamine + 2 mg/kg xylazine were determined during the quarantine process. The induction time was defined as the period from injection to NHPs achieving a recumbent posture. The recovery time was defined as the period from injection of atipamezole to the point when NHPs were climbing the iron bar in the cage. Total anesthesia time was defined as the time from the first injection (with tiletamine + xylazine) to the point when NHPs climbed the iron bar in the cage.
Computed tomography
After measuring the anesthesia times, the NHPs were anesthetized with ketamine 4 mg/kg + medetomidine 50 μg/kg intramuscularly for CT imaging (Biograph mCT Series PET/CT Scanner; Siemens Inc., USA) to determine the inner ear’s position for the subsequent mastoidectomy to treatment group. The CT imaging lasted 5 to 7 minutes under anesthesia. After imaging, the same volume of atipamezole, as an alpha-2 antagonist to medetomidine, was intramuscularly injected.
Anesthetic management during mastoidectomy
Four weeks after the CT scan, the NHPs were anesthetized with 8 mg/kg ketamine and 50 µg/kg medetomidine administered intramuscularly as premedication for isoflurane inhalation anesthesia to treatment group. Intubation was performed using a 3.5-mm internal diameter endotracheal tube after confirming complete relaxation of the intercostal and abdominal muscles and loss of the pupillary light reflex. Then, the surgery was performed under 2% isoflurane anesthesia with 100% oxygen (2 L/min) after confirmation of deep anesthesia with loss of the palpebral reflex. Mastoidectomy was performed for approximately 2 hours to administer the new drug to the inner ear. The surgical procedure involved making an incision to the skin and subcutaneous layer behind the auricle, followed by hemostasis to control bleeding. Next, mastoidectomy was performed using a high-speed drill to access the inner ear. The external auditory canal walls and eardrum remained intact throughout the procedure. Following confirmation of the presence of the round window and stapes, a 30 G Hamilton syringe was connected to a microinjector and utilized to administer the viral vector (2 × 1011 vg) of 10 μL via a slow injection through the pierced round window membrane. The purpose of viral vector administration in this study was to confirm its proper distribution in the inner ear 4 weeks later to treat hearing loss. We conducted this surgical procedure to initiate preclinical evaluation of the drug candidate, as there is currently no definitive treatment for hearing loss.
Veterinary postoperative care
After the surgery, the NHPs received veterinary postoperative care. Povidone-iodine (10%) was applied to disinfect the surgical site twice daily, with an intramuscular injection of enrofloxacin 5 mg/kg and subcutaneous injection of meloxicam 0.2 mg/kg twice daily for 14 days to prevent infections and relieve pain. Pain was further alleviated with an intramuscular injection of tramadol 2.2 mg/kg 4 times daily for 3 days and a subcutaneous injection of meloxicam 0.2 mg/kg twice daily for 14 days after the surgery. During these injections, the NHPs were restrained with a squeeze back. Body weights were measured once a week for 4 weeks after the surgery. The caloric intake from all feeds and foods consumed by the NHPs was calculated to determine if they consumed 100 kcal/kg body weight per day [23].
Statistical analysis
The Kruskal-Wallis test was performed to analyze all data as they did not meet the normality criteria. A p-value of <0.05 was considered statistically significant. Data are presented as mean ± standard deviation.
Results
Quarantine
During the 33-day quarantine period, physical examinations revealed no abnormalities indicative of infectious diseases, and no specific clinical symptoms were observed. Although abrasions of the ear canal and mild corneal damage were observed during physical examinations, no other clinical signs of infectious diseases were present. No major infectious microorganisms reported in NHPs were identified through microbiological examinations. Initially, food intake was low, but it gradually increased and normalized by the last quarantine day. Complete blood count, biochemical analysis including urinalysis, and dental findings were normal. Weight on days 15 and 30 did not decrease by more than 10% each compared to weight on day 1, with no significant difference compared to weight on day 1 (Fig. 1). On average, the daily caloric intake increased to > 100 kcal/kg body weight for the first time on day 19 (Fig. 2).
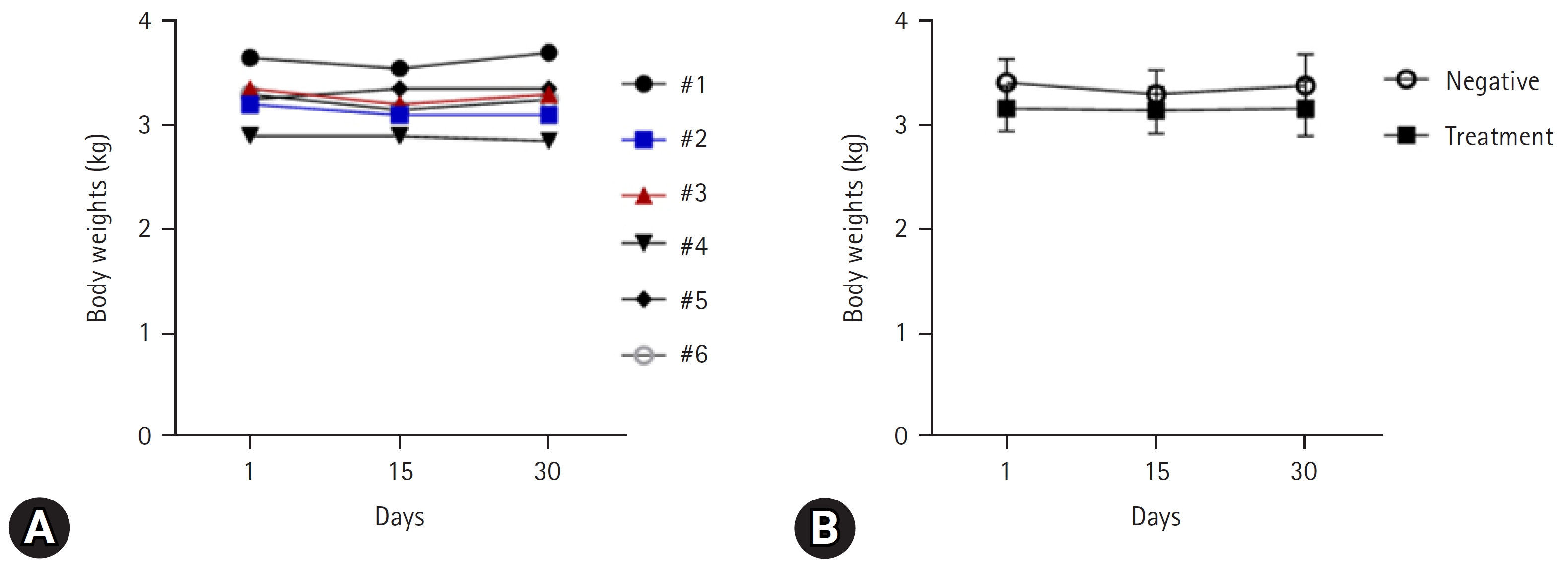
Body weight change in the quarantine period (A) by individual (6 females) and (B) on average (3 females per group). Data are presented as mean ± standard deviation.
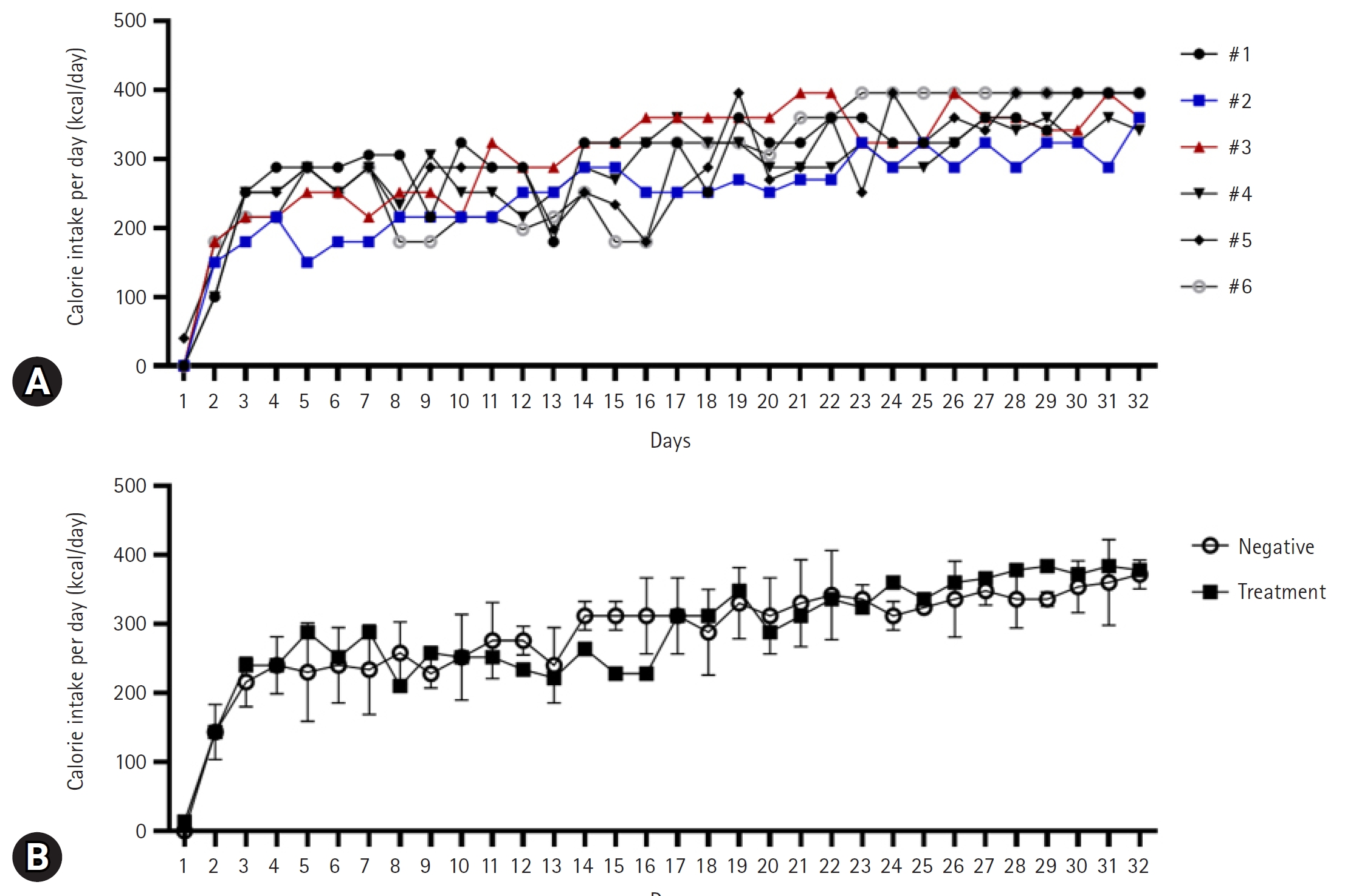
Calorie intake per day in the quarantine period (A) by individual and (B) on average (3 females per group). Data are presented as mean ± standard deviation.
Anesthesia for each experiment
When using 4 mg/kg tiletamine + 2 mg/kg xylazine, the induction time was 7.34 ± 0.58 minutes and total anesthesia time was 78.67 ± 10.02 minutes, with a Guedel’s classification of plane III, stage 3 anesthesia.
For 2 mg/kg ketamine + 50 µg/kg medetomidine, the dose did not induce recumbency and induction time could not be measured. For 4 mg/kg ketamine + 50 µg/kg medetomidine, the induction time was 7.67 ± 2.08 minutes and recovery time was 3.33 ± 0.58 minutes, with a Guedel’s classification of plane I, stage 3. For 6 mg/kg ketamine + 50 µg/kg medetomidine, the induction time was 6.33 ± 1.16 minutes and recovery time was 3.33 ± 0.29 minutes, with a Guedel’s classification of plane I, stage 3; the dose did not satisfy the criteria for plane II anesthesia due to the presence of corneal and laryngeal reflexes. For 8 mg/kg ketamine + 50 µg/kg medetomidine, the induction time was 4.67 ± 0.58 minutes and recovery time was 4.33 ± 1.16 minutes, with a Guedel’s classification of plane III, stage 3, and complete relaxation of the intercostal and abdominal muscles and loss of pupillary light reflex (Table 1). Accordingly, 4 mg/kg ketamine + 50 µg/kg medetomidine was regarded the most suitable dose for CT examination and 8 mg/kg ketamine + 50 µg/kg medetomidine was most suitable for intubation for inhalation anesthesia. No significant difference was observed between any of the anesthesia methods or times.
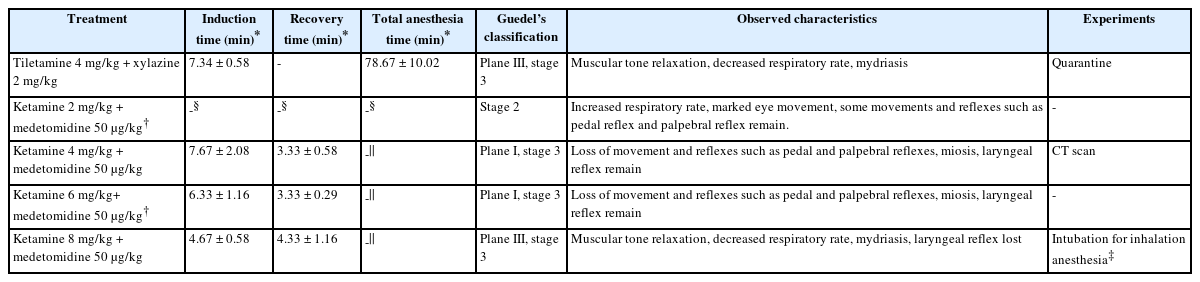
Induction, recovery, total anesthesia times, and Guedel’s classification according to anesthesia and anesthetic dose
Postoperative care
There were no infection-related factors or signs of inflammation at the surgical sites in NHPs. NHPs’ weights over weeks 1 to 4 did not decrease by more than 10% each week compared to their preoperative weight at all groups, and there were no significant differences compared with their preoperative weight at treatment group (Fig. 3). On days 1 and 4, the daily calorie intake significantly decreased compared with the preoperative weight at treatment group. On day 1, the daily calorie intake of treatment group significantly decreased compared with that of control group.
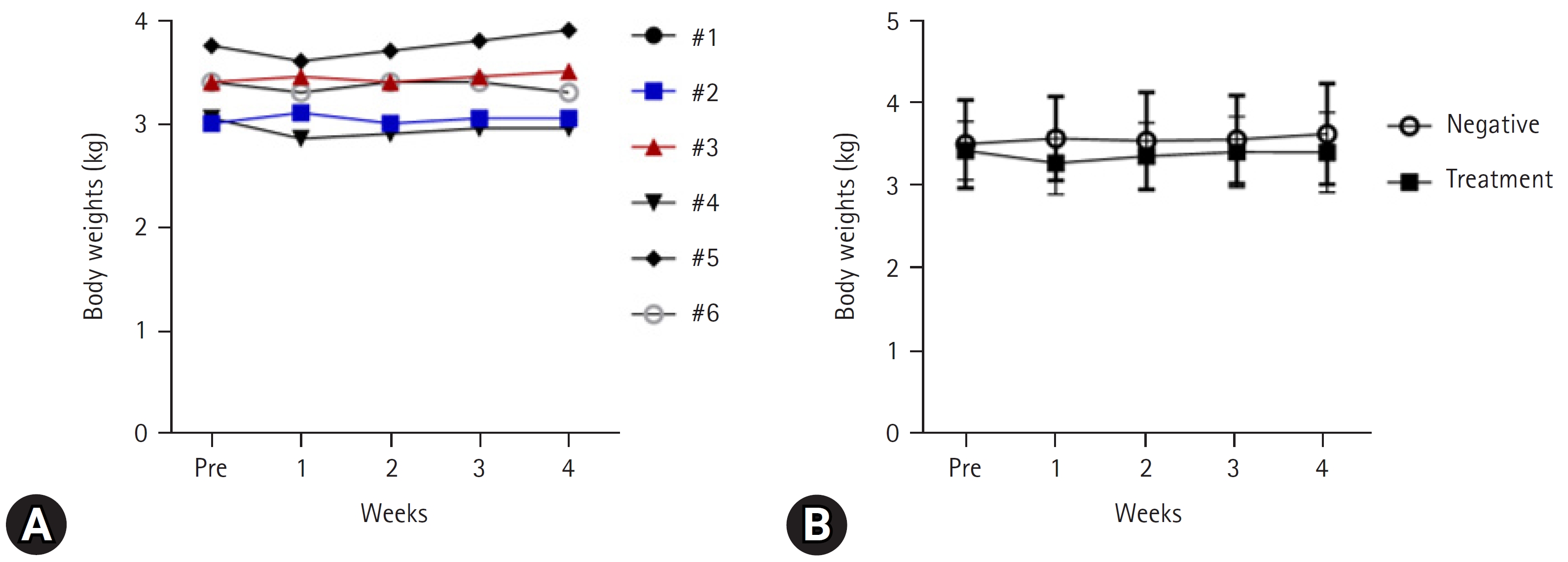
Change in body weight per day after surgery (A) by individual and (B) on average (3 females per group). Data are presented as mean ± standard deviation.
The daily caloric intake recovered to > 100 kcal/kg body weight for the first time on day 10 on average at treatment group (Fig. 4, Supplementary Table 1). There was no statistically significant difference in body weight across all groups and time points.

Change in feed intake per day after surgery (A) by individual and (B) on average (3 females per group). Data are presented as mean ± standard deviation (*p < 0.05 compared to pre, #p < 0.05 compared to control group).
Discussion
In this study, we described the veterinary management process for NPHs from the beginning to the end of an experiment. Following an advanced quarantine process, NHPs can be used in research after. We also used various anesthesia methods and doses for NHPs during quarantine, CT, and intubation for inhalation anesthesia. Additionally, post-invasive surgery, we administered appropriate veterinary care to alleviate pain and maintain body weight.
NHPs may serve as potential sources for the transmission of zoonotic infections. Therefore, the quarantine process is essential when studying NHPs in animal research facilities. However, previously applied quarantine programs have led to high morbidity and mortality owing to uncontrolled microbiological management and stress-induced immunosuppression [26].
To establish an effective quarantine process, a protocol was developed in the United States, which involved 2 or more PPD tests and a veterinarian’s physical examination at the beginning and right before the end of quarantine [26,27]. However, our quarantine process went beyond this regulation by implementing additional measures to strengthen the prevention of infectious disease spread. Our quarantine protocol included pre-education of researchers on zoonotic diseases, prior chest radiography of researchers, sterilization of items during transfer from the NHP area, showering before leaving the room, provision of an emergency kit, and monitoring of the presence of microorganisms inside the facility.
Experiments requiring anesthesia are diverse, but there is limited research on suitable anesthesia protocols, which can affect researchers’ choices. Therefore, researchers should understand the fundamental characteristics of anesthesia and customize the depth and duration as needed.
We determined different anesthetic drugs and doses for quarantine, CT, and mastoidectomy based on Guedel’s classification, which includes 4 stages and 4 planes. Among them, stage 3, characterized by intercostal muscle paralysis with diaphragmatic respiration, is suitable for surgery [28,29]. For quarantine, we aimed for plane III, Stage 3 anesthesia, lasting up to 60 min without the use of inhalation anesthesia. To this end, we selected tiletamine, an injectable anesthetic combination of equal volumes of tiletamine hydrochloride and zolazepam hydrochloride [30], with a longer anesthesia duration (45–60 minutes) when administered intramuscularly at 4 to 6 mg/kg compared to that of ketamine [30]. When combined with xylazine, tiletamine produces an anesthetic effect for 72 minutes [30,31]. Therefore, we selected intramuscular administration of 4 mg/kg tiletamine + 2 mg/kg xylazine as their total anesthesia time (78.67 ± 10.02 minutes) was sufficient for quarantine.
During the second and third anesthesia administrations conducted with a 4-week interval for CT and intubation for inhalational anesthesia, respectively, we used a combination of ketamine and medetomidine. Ketamine, a dissociative anesthetic, has a relatively rapid onset and shorter duration of anesthesia than other anesthetics [32]. To achieve a faster and deeper anesthesia induction and recovery while minimizing adverse effects and side effects, ketamine can be combined with medetomidine, which markedly potentiates the action of most anesthetic drugs [33–36]. The anesthesia methods at the second and third administrations were selected by evaluating the plane of anesthesia in stage 3.
For CT examination, we required short immobilization and rapid recovery of up to only 7 minutes. Therefore, 4 mg/kg ketamine with 50 µg/kg medetomidine were selected. To rapidly reverse the effects of medetomidine on the central and peripheral alpha-2 receptors, atipamezole was used at the same volume as medetomidine.
For intubation during mastoidectomy, we required short immobilization and a weakened laryngeal reflex. Therefore, we selected 8 mg/kg ketamine with 50 µg/kg medetomidine. This combination also avoided the side effect of nausea/vomiting after mastoidectomy. Demiroz Aslan et al. [37] reported that the group that received ketamine was more stable during mastoidectomy than the other group. This may be attributed to ketamine's ability to maintain stable hemodynamics, suppress hypotension, provide analgesia, and facilitate better intubation conditions, which may inhibit nausea/vomiting after mastoidectomy. Additionally, ketamine demonstrates effective analgesia, and medetomidine also possesses mild analgesic effects, making them suitable drugs for invasive surgeries [38,39].
After mastoidectomy, NHPs refrained from eating. They were provided with a wide variety of foods to ensure a daily calorie intake of 100 kcal/kg body weight and that did not lose more than 10% of their preoperative body weight [23]. If the provided food was not consumed by the NHPs for approximately 2 days, it was replaced with another food, and intake of as much protein as possible was promoted. As a result, the weight of each NHP decreased by only approximately 4.4% on average compared to the preoperative weight, and subsequently, it either increased or remained stable. Therefore, we determined that our body weight management was successful. Particularly, NHP #2 had difficulty in consuming pellet-type solid feed due to partial facial paralysis that occurred as a side effect of mastoidectomy. Therefore, she was provided with human formula, and her body weight increased.
Accurately recognizing nonverbal expressions of pain in laboratory animals is important, and effective pain assessment methods are necessary for their welfare [40]. Particularly, after invasive procedures such as surgical incisions, sensitivity to pain can increase in the traumatized area and its surrounding tissues. Although not always evident, careful observation of changes in appearance and behavior over time can help identify signs of pain. In particular, NHPs capable of expressing emotions through facial expressions should be closely observed for grimacing [40]. These observations will aid in the accurate evaluation of pain after experimental procedures.
To alleviate postoperative pain, a combination of meloxicam (0.2 mg/kg subcutaneously twice daily) and tramadol (2.2 mg/kg 4 times daily) was administered. Meloxicam, a nonsteroidal antiinflammatory drug, has been used to control postoperative pain in combination with opioids [41]. The combination of nonsteroidal antiinflammatory drugs and opioids is frequently used for synergistic analgesic effects on acute and chronic pain [42]. Long-term tramadol treatment for > 3 days is prohibited to prevent drug tolerance [43]. Therefore, we administered tramadol for only 3 days and then administered meloxicam alone to manage pain. Additionally, NHPs exhibited squatting behavior and touched the surgical site until day 3; these behaviors are indicative of pain and discomfort in NHPs [44]. However, these behaviors were no longer observed after day 4, and calorie intake per day recovered to approximately 200 kcal/day on day 3, resulting in the discontinuation of tramadol.
The present study describes the anesthesia technique and postoperative management for mastoidectomy, an invasive surgery. Although the specific details may vary for other types of invasive surgery, the monitoring methods, anesthesia duration, and analgesic selection reported in this study can be applied to other studies as well. Therefore, our findings can contribute to the development of standardized anesthesia protocols for various invasive surgical procedures.
One limitation of this study is the lack of quantitative pain evaluation, such as the Grimace pain scale or cortisol blood level measurement. Therefore, we were unable to fully assess the extent of pain experienced by the animals and the effectiveness of pain management. In future experiments, it would be essential to establish a protocol for pain evaluation and management. This would allow for a more comprehensive understanding of the pain experienced by the animals and enable us to develop more effective pain management strategies.
Notes
The authors declare no conflict of interest.
Acknowledgements
This research was funded by the Daegu-Gyeongbuk Medical Innovation Foundation in 2020 (project no. L22008 and R22048).
Supplementary Materials
Supplementary data are available at https://doi.org/10.14405/kjvr.20230032.
Food intake of postoperative care after mastoidectomy