
Extracranial hematomas can be widely divided into three types, depending on its location; cephalohematomas, subgaleal hematomas, and caput succedaneum in human medicine [1]. Subgaleal hematomas are rare but potentially lethal condition found in newborns in humans [2]. They occur due to the tearing of emissary veins between the dural sinuses and scalp veins, and are not limited by suture lines [2,3]. Subgaleal hematomas form within the potential space between the periosteum and the galea aponeurosis, which is a tough fibrous tissue beneath the skin and subcutaneous tissue [1,3].
Cephalohematomas are calvarial subperiosteal hematomas that typically occur in the subperiosteal space and are confined by suture lines, meaning they cannot cross the midline [1,4]. Caput succedaneum is a subcutaneous serosanguineous fluid collection external to the galea aponeurosis. It extends across the midline and over suture lines [5].
Subgaleal hematomas are rare but potentially lethal condition. If it occurs, unlike other extracranial hematomas, infants may lose up to 50% of their blood volume into the subgaleal space [6]. Additionally, it requires careful monitoring for thrombocytopenia and coagulation studies. Thus, it is important to differentiate this type of hematoma from other extracranial hematomas.
There were some reports of extracranial hematoma diagnosed by variable imaging findings in humans. In veterinary medicine, however, there are few reports of extracranial hematoma. Therefore, subgaleal hematoma may be underdiagnosed in veterinary medicine for cases of head trauma. The purpose of this report is to apply the concept of extracranial hematoma in veterinary medicine and to describe the imaging features of a subgaleal hematoma induced by a traumatic event in a dog.
A 2-year-old male Chihuahua was presented with a severe head swelling. There was extensive circumferential swelling of the entire scalp immediately after bumping his head into the other dog. The dog showed delirium and respiratory distress. Pain reaction was observed when the swelling scalp was palpated. The patient had no other neurological deficits and modified Glasgow coma scale score was 17. Vital signs indicated a normal heart rate of 88 beats per minute, a normal systolic blood pressure of 114 mmHg, an elevated respiratory rate of 90 per minute, and capillary refill time was less than 2 seconds. A complete blood cell count and serum biochemical analysis revealed a mild reduction in the red blood cells (3.35 [106/μL], reference range 5.5 to 8.5 [106/μL]) and hematocrit (22%, reference range 39%-56%).
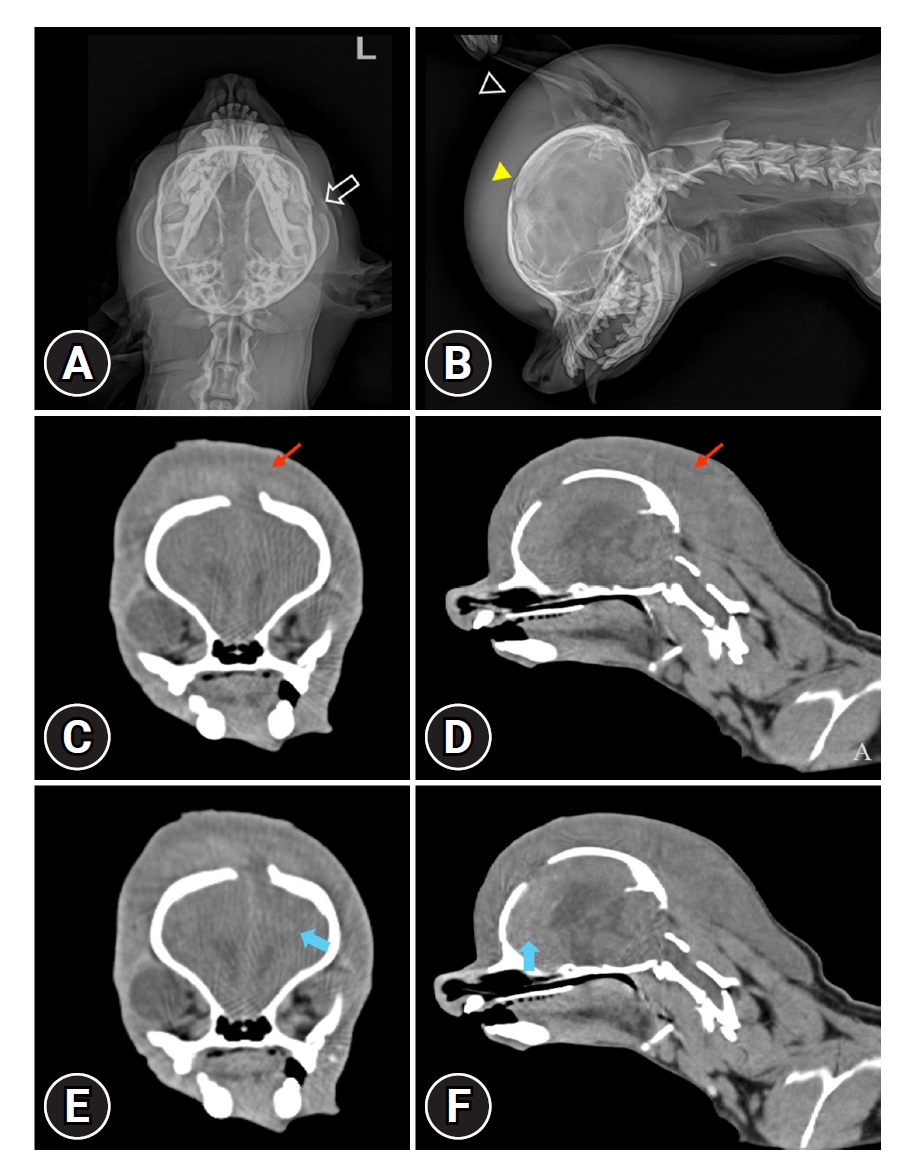
The radiography of skull revealed extensive, circumferential soft tissue swelling from entire skull to dorsal region of 2nd cervical vertebrae (Fig. 1A and B). Additional radiographic findings included open fontanelle and fracture of left zygomatic arch.
The computed tomography (CT) examination (Alexion; Canon Medical Systems, Japan) was performed for accurate diagnosis and evaluation of intracranial hemorrhage, intracranial hypertension, and additional skull fracture. Because the mental state was delirium, the patient was positioned in ventral recumbency without anesthesia. The CT parameters were 120 kilovoltage peak, 150 milliampere seconds, 1.0mm slice thickness, 1.0 mm interval, 0.75 second rotation time, and 0.938 collimation beam pitch. Post-contrast CT images were acquired at 90 seconds after intravenous injection of 600 mg iodine/kg iohexol (Omnipaque; GE Healthcare, Ireland). CT revealed a massive swelling encircling the entire calvarial vault, extending toward the cervical neck and crossing the suture line. It was heterogeneously, mild hyperdense fluid to soft tissue attenuating with a mean of 37 HU (range of 27-48 HU). The top differential diagnosis was a subacute phase hemorrhage, but the possibility of edematous change of scalp tissue or abscess could not be ruled out. There was also mild hyperdense lesion in left frontal lobe suspected intracranial hemorrhage and contusion. It had a mix of mildly contrast enhancing portions (30-55 HU) (Fig. 1C-F).
Laboratory examination showed no thrombocytopenia and normal coagulation studies. Mannitol 1 g/kg/IV for 30 minutes, vitamin K and diazepam 0.5 mg/kg/IV were administered for preventing seizure considering the location of intracranial hemorrhage.
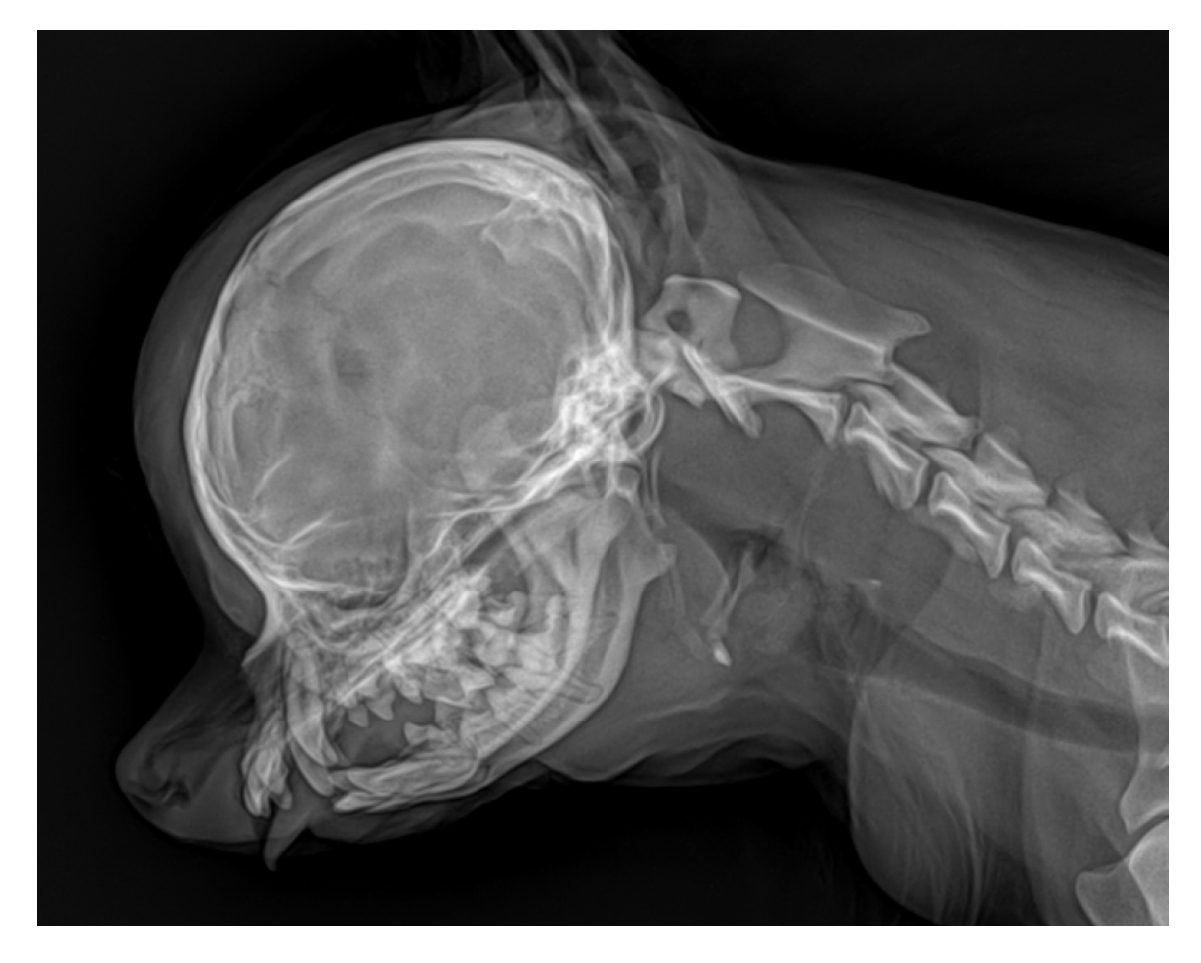
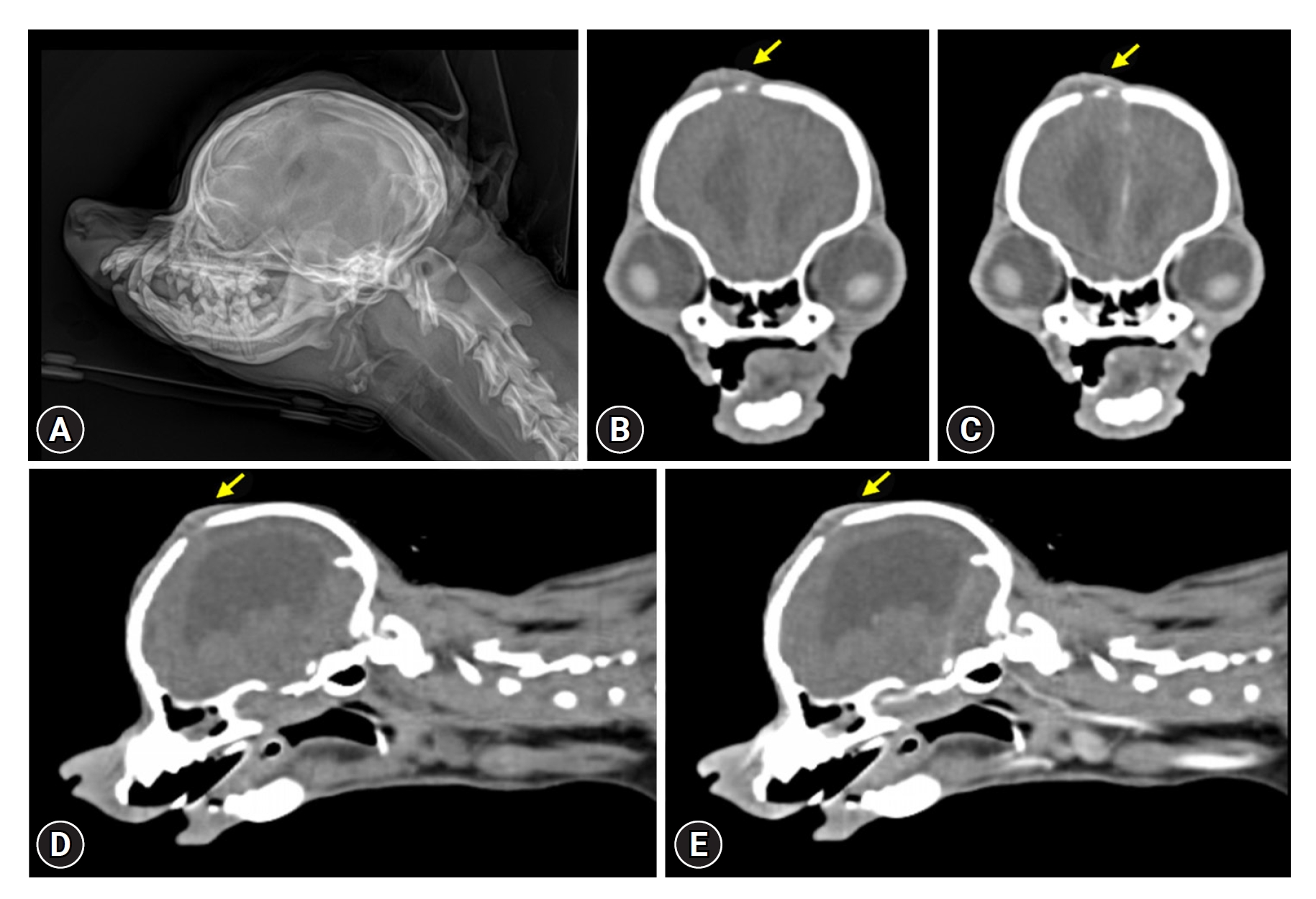
On day 2, the dog had improved appetite and mental status and could sit voluntarily. The respiratory status and the swelling of the skull were progressively improved by day 4 (Fig. 2). On day 24, follow-up radiography and CT examination was performed and revealed significant interval improvement in the subgaleal hematoma, leaving behind a small residue at frontal bone level (Fig. 3).
Subgaleal hematoma is a rare and potentially life-threatening condition in newborns and children in human medicine [1,2]. It is an accumulation of blood in the space between the periosteum and the epicranial aponeurosis, due to the rupture of the emissary veins [2]. Subgaleal hematomas are often encountered in parturitional injury, but may also occur spontaneously or secondary to traumatic events [7,8]. Clinically, it reveals diffuse and boggy swelling of scalp [9]. Subgaleal hematoma and caput succedaneum can be mistaken for each other, as both can also extend across the suture lines, but swelling of caput succedaneum resolves more rapidly (within the first 12-18 hours) [2]. Subgaleal hematomas typically resolve within a few days to weeks, and in cases of massive bleeding or associated complications, surgical drainage may be necessary [3]. If it occurs, unlike other extracranial hematomas, infants may lose up to 50% of their blood volume into the subgaleal space [6]. Thus, it is important to differentiate these types of extracranial hematomas by performing CT and magnetic resonance imaging (MRI). If a subgaleal hematoma is diagnosed, careful monitoring for hypovolemia and additional laboratory examinations, such as for thrombocytopenia and coagulation studies, are necessary. Additional information such as intracranial hypertension, intracranial hemorrhage, and skull fracture can be obtained by performing CT and MRI.
CT features of subgaleal hematomas in humans include heterogeneous, mildly contrast enhancing portions, similar to the dog in this case. The CT features of cephalohematoma include a hypo- to hyperdense mass. However, cephalohematomas can be differentiated from subgaleal hematomas because they are typically located in the parietal or occipital region of the calvarium and cannot cross the suture line [2]. Cephalohematomas were also often characterized by a mineralized outer rim [1,4,10]. The CT features of subgaleal hematoma are also distinguished from those of caput succedaneum, as subgaleal hematomas are more extensive lesion compared to caput succedaneum [5,11]. Subgaleal hematomas are located in subaponeurotic space, which is a potential space extending anteriorly to the orbital margins, posteriorly to the nuchal ridge, and laterally to the temporal fascia [11]. Therefore, while a subgaleal hematoma can extend toward the posterior neck along the superficial neck fascia, caput succedaneum typically occurs as a localized 'bump' at the vertex of the skull [5,11].
In human medicine, MRI is frequently performed for the diagnosis of extracranial hematomas, including a subgaleal hematoma [12]. On MRI, subgaleal hematoma is identified as blood accumulation between the periosteum and the galea aponeurotica. It is typically observed in a diffuse, massive form or capsulated shape not confined to the suture line. Similar to intracranial hemorrhage on MRI, the T1-weighted and T2-weighted signals vary depending on the age of the hemorrhage. Despite the higher anesthesia risk, MRI offers the advantage of accurate evaluation of extracranial hematoma types. However, CT, similar to typical traumatic brain injury cases, has the advantage of minimal anesthesia limits and allows for rapid assessment of hematoma and extension over the suture line. In our case, only CT was performed for evaluation due to the high anesthesia risk and the patient not being under anesthesia.
In the human literature, intervening on subgaleal hematomas is rarely necessary in children [3]. The clinical signs of pain and swelling usually resolve within a few days to weeks and surgical drainage is rarely needed. When the complications are suspected, however, surgical drainage may be necessary [3,4,7]. Airway compression [13], orbital compartment syndrome [6], infection [14] has been reported as potential complications of traumatic subgaleal hematomas in humans. Orbital compartment syndrome, especially, has commonly been described with extension of the hematoma to the orbital subperiosteum [6]. In our case, we thought that prompt surgical drainage of the hematoma was not required.
Subgaleal hematomas are most often in newborns attending the delivery room in human [1,2,5,9]. The condition is much rarer in older children and adults [3,4]. In older children, minor head injury, hair pulling or braiding, trauma leading to a skull fracture can cause subgaleal hematoma [4,6,7,14]. There are current two veterinary reports of subperiosteal hematoma [1,15]. In the two reports of subperiosteal hematomas, the patients were juvenile with the oldest being 6 months, and our case was 2-year-old adult dog. This suggests the importance of expanding the differential diagnosis to include adult dogs in veterinary medicine as observed in humans.
Histopathology of the calvarial lesion was performed in a dog with subperiosteal hematomas [1]. In that case, the histopathologic findings were showed collagenous fibrous connective tissue interspersed with a moderate number of reactive fibroblasts and a moderate neovascularization as well as multifocal areas of hemorrhage. It was suggested to a periosteal reaction and remodeling hematoma. If circumstances allow, confirmation through histopathology is recommended. However, we considered that confirmation of extracranial hematoma can be sufficient through fine needle aspiration and MRI regarding the location and composition of the hematoma.
This report has some limitations. First, fine-needle aspiration was not performed to confirm hemorrhage. There was no pain reaction during palpation, and blood examination indicated no need for drainage. CT findings were similar to those of a subgaleal hematoma. Consequently, confirmation of swelling and hemorrhage could not be achieved. Second, due to the dog's delirious mental state and respiratory distress, we were unable to proceed with an MRI. Therefore, we could not differentiate the types of extracranial hemorrhages and confirm whether blood had accumulated between the periosteum and the galea aponeurotica on MRI.
In this report, subgaleal hematoma was suspected in an adult dog with a head trauma, and the imaging features were described. In conclusion, extracranial hemorrhage including subgaleal hematoma, caput succedaneum, and cephalohematoma should be considered as differential diagnosis when the dog have extensive soft tissue edema of the skull with a history of head trauma. Imaging examinations including radiography, CT, and MRI could be useful for differential diagnosis of extracranial hematomas. If a subgaleal hematoma is diagnosed, careful monitoring for hypovolemia and additional laboratory examinations, such as for thrombocytopenia and coagulation studies, are necessary.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print







